Introduction
Vertigo is a significant symptom often confused with diagnosis. ENT surgeons and neurologists play a major role in the diagnosis of vertigo. Usually, we are at a lack of evidence in the diagnosis of vertigo so a thorough search through history and examination is essential to the diagnosis and management. This is one of the few symptoms where evidence seems to vary with time. The commonest cause of vertigo in adults is BPPV (1) and this condition requires further tests to know which side and which semicircular canal is affected. This complicates the diagnosis but fortunately, we find that patients commonly have posterior canal BPPV so the diagnosis is simple. When a variation occurs in the position then the skills of the otoneurologist are put to the test and this requires learning and patience. The posterior SCC is involved in 80% of the cases and the anterior SCC in 5%of the instances. Katsarkas described the anterior SCC BPPV in 1987 (2). The anterior BPPV can clinically be suspected when in the dix-Hallpikes test there is a vertical down-beating paroxysmal nystagmus in the head hanging method which remains even in sitting posture. The nystagmus has all the components of peripheral nystagmus like latency, fatigability, directionally opposite and reduced repeatability. This anterior canal BPPV always confuses with apogeotrophic PSCC BPPV and can be decided when the torsional counterclockwise component is more prominent in the APO-GEO-PSC BPPV than the ASCC BPPV. The present study is to confirm the incidence and to differentiate through various means the anterior BPPV from apogeotrophic PSCC BPPV and others through the VHIT method. This method could quantify the differences in intensity, direction of nystagmus, triggering positions and inversions during return to sitting position, and can all be measured. This helped us in determining the involved SCC and also to direct appropriate manoeuvres to settle the malady.
Aims and objectives
This is a retrospective study involving the authors with vestibulology experience.
(1) to consider and diagnose ASCC BPPV
(2) to differentiate ASCC BPPV from apogeotrophic PSCC BPPV (1, 2)
(3) to use VHIT as a documentary evidence for diagnosing BPPV.
Materials and methods
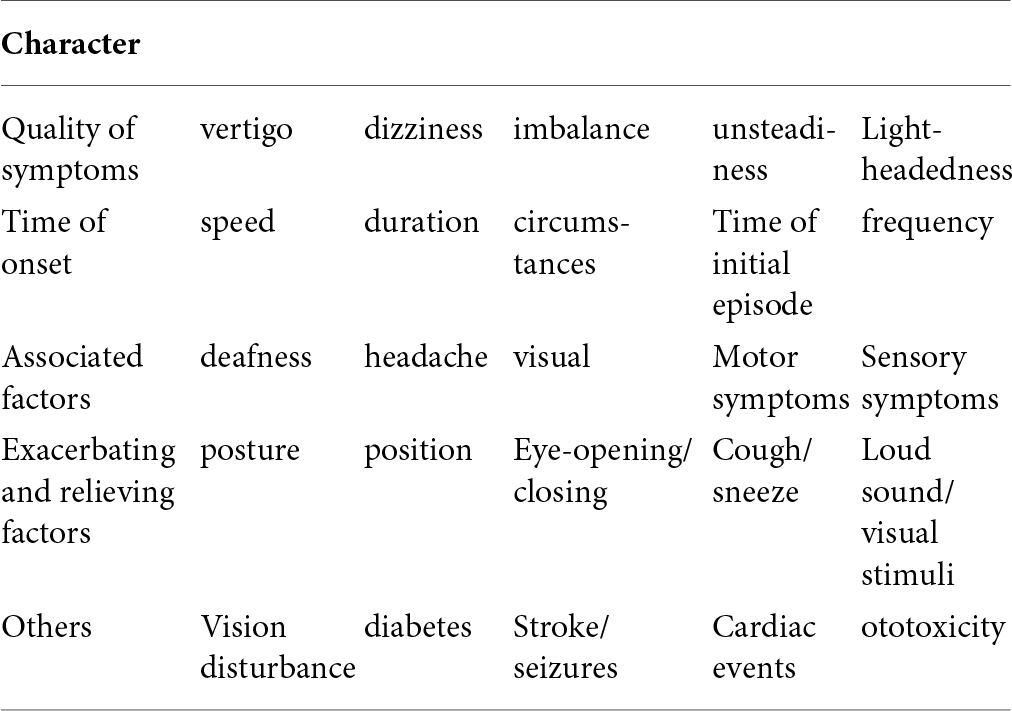
The study was done between 2015–16 and about 227 patients took part in the study after obtaining proper consent for diagnosis and treatment in a tertiary medical centre. This study is a retrospective study which was double-blinded with about 117 symptomatic and another 110 normals who underwent the procedure without any symptoms. A few of the normal public also were shown to have variations implying a semicircular canal problem, but the symptoms of the patients when correlated with the exact VHIT finding did not correlate. There were 49 men and 68 women symptomatic patients in the study. the patients who presented in the OPD were properly documented and follow-ups of the patients were made either by direct visits or through telephonic contact. Our patients underwent a general checkup with audiometry, head hanging test, head shaking test, nystagmus examination, head thrust test, gaze test, hints test and positional vertigo was identified with Dix Hallpike’s manoeuvre and the patients were subjected to VHIT to document the semicircular canal. A proper case history is very important to differentiate positional from other causes of vertigo and to subject the patients to various investigations for a definitive diagnosis. In this regard, we applied a properly conceived case history and various manoeuvres to document the positional vertigo. The patients were initially thoroughly examined on the following clinical aspects (3).
All the patients underwent a VHIT test and the sign that was looked for was vertical downbeat nystagmus (4) and the torsional component was properly examined to differentiate from the apogeotrophic PSCC BPPV.
Out of the 117 patients, only four patients had symptoms similar to ASCC BPPV and the results were summarized. On VHIT exam, only two had positive anterior BPPV curves (1).
Case 1
A 63-year-old male a driver by occupation came to the hospital with complaints of a spinning sensation when he was bending forward in the sitting posture. Initially, the symptoms were mild which became severe over 2 months. He was a known diabetic on OHA but was not hypertensive. After a preliminary ENT examination, he was subjected to dix Hallpike manoeuvre but was positive for vertical downbeat nystagmus on the right side and was very suggestive. Audiometry and other investigations were negative. So we suggested him to undergo VHIT procedure. It showed the typical ASCC BPPV. A Yakovino’s manoeuvre was very helpful in relieving the symptoms.
Case 2
A 48-year-old lady came to the hospital with symptoms of a spinning sensation on getting up with vomiting she was a diabetic and hypertensive initial examination was wrongly diagnosed a posterior SCC BPPV but after the Epley’s manoeuvre was not relieved of the symptoms and it was aggravated and further examination found her to be negative for audiometry, CT scan, since she had symptoms more on getting up and also a forward position which was demonstrated in DHP Test, She underwent a VHIT which showed signs of anterior SCC BPPV. This patient did not have signs typical of apogeotrophic pscc BPPV also.
VHIT findings
Of the 227 patients who underwent the VHIT test, 117 were symptomatic. A total of 4 patients had signs of reduced vor gains (<0.8)anterior BPPV of which only two had symptoms typical of anterior BPPV (50%) Most of the patients had findings of posterior SCC and a few had lateral semicircular canal. About 10 patients had multiple canals vor reduced gains which were documented. Although the VHIT correlated well with the patient’s symptoms in SCC BPPV, the findings in some normal persons (no = 12) were not objective and were found symptomatically normal (p > 0.05). The Pearson’s r-value correlated well with the ascc to the clinical findings.
After the diagnosis, the patient was subjected to Yakovinos manoeuvre. Here irrespective of the side affected the patient is moved quickly in a straight head-hanging posture (5) and the head is tilted to 30* and kept for 30 s, later the patient is moved to a supine head-up posture with the forward inclination at 30*for another 30 s and finally the patient is moved to a sitting position with the head at 30* for 30 s. In PSCC APC patients, the qlr (quick liberatory manoeuvre) is done (2). When a patient has no nystagmus then the treatment is complete. The accuracy of the treatment is dependent on the diagnosis and the consequent manoeuvre. The straight-head hanging method produced the maximum velocity for the canalithiasis.
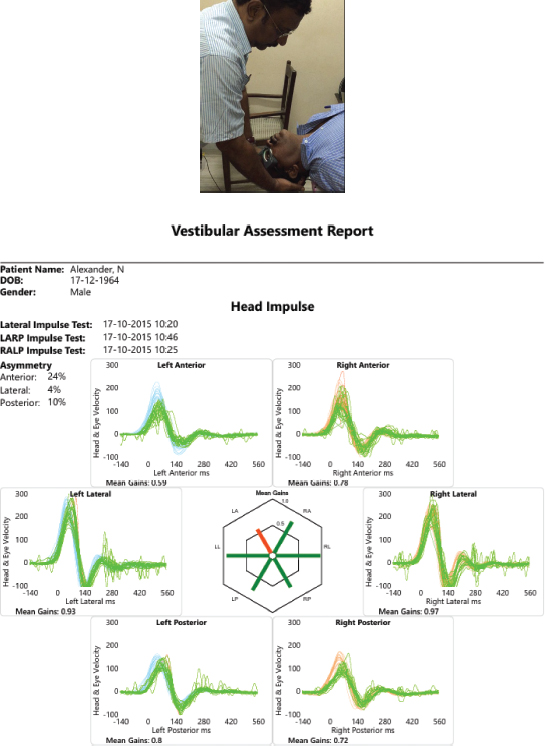
Left anterior SCC BPPV
All these patients underwent various particle reposition manoeuvres and the anterior BPPV patients underwent the Yakovinos manoeuvre successfully. Since the patient did not return for follow-up the VHIT was not performed to know the results after the Yakovinos manoeuvre.
Discussion
Anterior semicircular canal BPPV is rare but present and one should always have it in mind when the patient is presenting with a spinning sensation from a different perspective and also when Epley’s manoeuvre has failed. This is all the more important when certain neurological diseases like multiple sclerosis (6) or migrainous vertigo (7) present as ascc BPPV which can be clinically made out but should be confirmed by MRI.
The causes of BPPV may be many including trauma, idiopathic, prolonged one-sided sleep, inner ear disorders etc and the associated factors include women, age < 65, hypertension, diabetes mellitus, hyperlipidaemia, vitamin-D deficiency (8), and osteoporosis (4).
Clinically a vertical down-beating nystagmus is very typical of anterior BPPV, but the torsional component should always be looked into as well as the duration of the nystagmus. Vertical Downbeat nystagmus is itself a sign to be looked into carefully because it’s associated with many central neurological diseases (9). So any positional vertigo should have a central component analysed.
The pathophysiology is due to the dislodged otoconia like oc90, otolin and sc1 (5) which bind to calcium carbonate from the utricular macula into the semicircular canal which results in canalithiasis or cupulolithiasis. In 1969 Harold Shucknekt proposed the cupulolithisis in patients who have cupula with ca debris. Castelluci (10) proposed that there could be a partial or complete jam of the SCC resulting in the reduction in the VOR gain in patients with persistent BPPV symptoms and this should be thought of in long-standing cases. The bow and lean test helps in differentiating canaliohiasis (Epley) from cupulolithiasis where the nystagmus stays longer in the bow and lean test whereas in canalithiasis it disappears early. In our cases, we didn’t aspire to know the canalithiasis or cupulolithiasis as the patient improved over time. Newer developments in the form of short canal and long canal lithiasis and, the diameter of the common crus (11) have been the current scenario. The oculomotor pattern in VHIT shows promise in differentiating between closely similar canalithiasis (12). In 2 cases of supposedly anterior canal BPPV there was no nystagmus and so was the VHIT. These patients presented with vertigo when leaning forward and were progressively increasing in intensity and duration. The patient was treated outside with failed epleys manoeuvre and so was referred to our institution. When we took the history it was amply evident that it was a case of ascc BPPV and the VHIT typically showed reduced VOR Gains in the VHIT. The Yakovinos manoeuvre proved to be effective in treating the patients. Only two patients out of 117 were found to have ASCC BPPV(2%).this less well correlated with international statistics where the incidence is higher. Similarly, we made out apogeotrophic PSCC BPPV in 4 cases as the patients were already suffering from pscc BPPV. This was also interpreted better with VHIT as these patients not only had torsional component variation according to the side but also oculomotor variations in the VHIT.
It has been found that 2.4 % of all people undergo BPPV in their lifetime (5).
Conclusion
The series of cases in our study proves that there is good evidence to diagnose rarer forms of BPPV and the efficacy of the consequent treatment through VHIT. A bow and lean test with dix-Hallpike manoeuvre helps a great deal in the diagnosis of most BPPV (13). The clinical diagnostic manoeuvres in the form of vertical or horizontal, downbeat or upbeat, torsional strength of the nystagmus goes a long way in properly diagnosing BPPV (9) and various diagnostic manoeuvres and the documentation through VHIT further confirm the need for further research with this instrument.
References
1. Ghosh A, Dorasala S. Epidemiology of benign paroxysomal positional vertigo (BPPV) and risk factors for secondary BPPV: a population-based study. Egypt J Otolaryngol. (2023) 39:93. doi: 10.1186/s43163-023-00456-6
2. Califano L, Salafia F, Mazzone S, Melillo MG, Califano M. Departmental Unit of Audiology and Phoniatrics “G. Rummo” Hospital, Benevento, Italy. Acta Othorinolaryngol Ital. (2014) 34:189–97.
3. Bhandari A, Bhandari R, Kingma H, Strupp M. Diagnostic and therapeutic maneuvers for anterior canal BPPV canalithiasis: three-dimensional simulations. Front. Neurol. (2021) 12:740599. doi: 10.3389/fneur.2021.740599
4. Porwal P, Pawar V, Dorasala S, Bijlani A, Nair P, Nayar R. Clinical and VNG features in anterior canal BPPV—an analysis of 13 cases. Front. Neurol. (2021) 12:618269. doi: 10.3389/fneur.2021.618269
5. El-Anwar MW, Mesriga RMKM, Mobasher MA, Heggy M, Meky A, Nofal AA. Benign paroxysmal positional vertigo: a multi-center study. J Neurol. (2021) 268:1995–2000. doi: 10.1186/s43163-022-00295-x
6. Musat GC, Musat AAM. Multiple sclerosis presenting as an anterior semicircular canal benign paroxysmal positional vertigo: Case report. Ear Nose Throat J. (2021) 100:636S–40S. doi: 10.1177/0145561319897983
7. von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, et al. Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry. (2007) 78:710–5. doi: 10.1136/jnnp.2006.100420
8. Kim HJ, Park J, Kim JS. Update on benign paroxysmal positional vertigo. J Neurol. (2021) 268:1995–2000. doi: 10.1007/s00415-020-10314-7
9. Bertholon P, Bronstein AM, Davies RA, Rudge P, Thilo KV. Positional down beating nystagmus in 50 patients: cerebellar disorders and possible anterior semicircular canalolithiasis. J Neurol Neurosurg Psychiatry. (2002) 72:366–72. doi: 10.1136/jnnp.72.3.366
10. Castellucci A, Malara P, Martellucci S, Armato E, Califano L. Possible pathomechanism behind the transient hypofunction of the affected canal in BPPV. Letter to the editor regarding “Clinical significance of video head impulse test in benign paroxysmal positional vertigo: a meta-analysis” by Elsherif M et al. European Archives of Oto-Rhino-Laryngology (2021);278(12):4645-4651. Eur Arch Otorhinolaryngol. (2022) 279:1117–8. doi: 10.1007/s00405-021-07202-9
11. Korres S, Riga M, Sandris V, Danielides V, Sismanis A. Canalithiasis of the anterior semicircular canal (ASC): treatment options based on the possible underlying pathogenetic mechanisms. Int J Audiol. (2010) 49:606–12. doi: 10.3109/14992021003753490
12. Cole SR, Honaker JA. Benign paroxysmal positional vertigo: effective diagnosis and treatment. Cleve Clin J Med. (2022) 89:653–62. doi: 10.3949/ccjm.89a.21057