Introduction
A Global cancer observatory published in May 2019 (1) observed an incidence of 2.2% carcinoma hypopharynx, 2.5% carcinoma larynx, and 1.5% carcinoma oropharynx. Diagnosis and follow-up of these patients are done by examination with videolaryngoscopy (VLS). Hopkin rods have greatly enhanced the magnification and depth for detailed observation during examination of the larynx; they have also been modified to view from different angles. The use of VLS has reserved direct laryngoscopy for therapeutic purposes. We did a study intended to analyze the VLS findings and the find annual percentage prevalence of carcinoma larynx, hypopharynx, oropharynx and its subsites, as well as assess the effectiveness of videolaryngoscopy for diagnosis and follow-up.
Materials and methods
All patients who attended ENT OPD and diagnosed with later biopsy-proven carcinoma and patients referred from oncology department after chemoradiotherapy for follow-up were included in the study. Videolaryngoscopy was done using a 45-degree Hopkins rod nasal endoscope, with the patient sitting with tongue held in hand. The period of study was April 2023 to March 2024 and the type of study was analytical cross-sectional. Institutional ethical committee clearance was obtained. There are no conflicts of interest.
Results
A total number of 132 patients underwent videolaryngoscopy in 1 year (Table 1 and Figure 1).
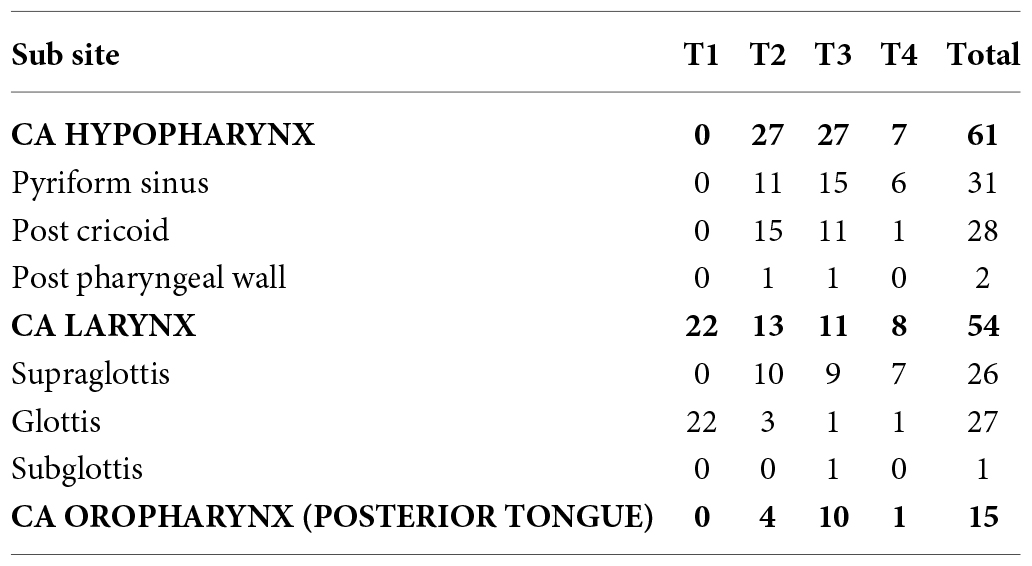
Table 1. Summary of cases.
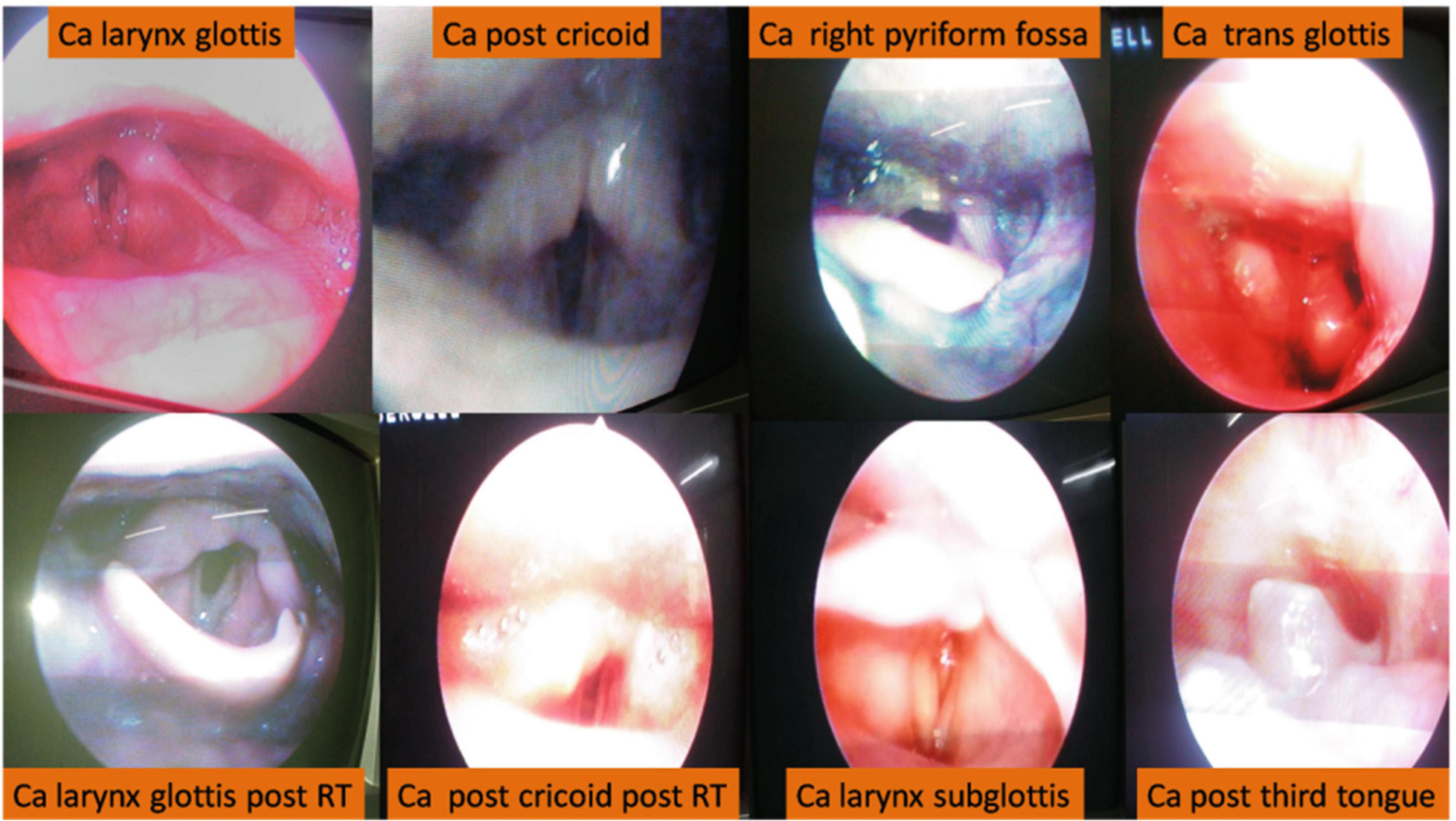
Figure 1. Videolaryngoscopic findings.
Carcinoma hypopharynx
Carcinoma hypopharynx was diagnosed in 61 patients. Among them, cases of carcinoma involving Pyriform fossa were 32 (Male–26, Female–6), carcinoma Post cricoid were 27 (Male–7, Female–20), and carcinoma of posterior pharyngeal wall were 2 male patients. Among the 32 cases of pyriform fossa malignancy, 17 cases were on right side and 15 cases had a left side lesion, and the clinical staging was T1 = 0, T2 = 11, T3 = 14 and T4 = 7. The symptoms were Dysphagia = 22, Ear pain = 5, Throat pain = 3, Stridor = 3, Neck swelling = 1 and Foreign body sensation = 1. VLS was done for diagnostic purposes in 16 patients who had T2 = 5, T3 = 8, T4 = 3 lesions and biopsy was done for all. VLS was done for follow-up in 16 patients after chemoradiotherapy. 6 patients with T2 lesion previously had no symptoms, 10 patients had persistence of symptoms even after chemoRT. Among the 27 postcricoid malignancies, 26 were in the midline with T1 = 0, T2 = 15, T3 = 11 and T4 = 4. Symptoms were Dysphagia = 27, Voice change = 3 and Dyspnea = 1. VLS was done for Diagnostic purposes in 4 cases. But VLS could not diagnose growth in post-cricoid. Only vocal cord or arytenoid involvement and pooling of saliva are visualized in VLS. All cases underwent a biopsy by flexible UGI scopy. VLS was done for follow-up in 23 cases after chemoradiotherapy. 12 patients had no symptoms, while 11 patients had persistent Dysphagia. There were two cases of posterior pharyngeal wall was midline, with 1 each T2 and T3. The symptom was Dysphagia in both. VLS was done in one for diagnosis and a biopsy was taken. VLS was done for follow-up in one, had persistent Dysphagia, with edema of arytenoids.
Carcinoma larynx
There were 54 patients with carcinoma larynx. 26 patients had supraglottis malignancy (Male–22, Female–4). Among them, 10 had T2 lesion, 9 had T3 lesion, and 7 had T4 lesion. Symptoms were Dysphagia–10, Voice change–7, Throat pain–8, and Stridor–2. Among 26 patients, 10 patients had ventricular band growth. Diagnostic VLS was done in 5 patients. In all cases, biopsy was done with VLS and they were referred for chemo RT. Follow-up VLS was done for 5 patients after chemo RT, 2 patients had no symptoms while 3 patients had persistence of symptoms. The other 16 patients with supraglottis malignancy had epiglottis growth. Diagnostic VLS was done in 10 patients. Biopsy was done with VLS for all and they were referred for chemo RT. Follow-up VLS was done for 6 patients after chemo RT. 5 patients had persistent of symptoms, 1 patient had no symptoms and no lesion. 27 patients had Glottis malignancy (Male–22, Female–5). Symptoms were voice change in 13patients and hoarseness of voice in 14 patients. Diagnostic VLS was done in 5 patients and 3 were prepared for microlaryngeal biopsy, while biopsy was done with VLS in 2 patients. Follow-up VLS was done for 22 patients after chemo RT. 13 patients had no symptoms and there was no evidence of lesion, and 9 patients had persistent symptoms of edema and thickening. 1 patient, a known Ca oropharynx T3, had Chemo RT 1 year ago, then presented with Stridor found to have a subglottic growth T3 lesion (2nd primary). Tracheostomy was done, later planned for microlaryngeal biopsy.
Carcinoma oropharynx
15 patients of posterior 1/3rd tongue growth underwent VLS. Tonsillar fossa growth cases were not included in study. There were 11 Males and 4 females. Lesion was on midline in 12, Right in 2, and left in 1. Symptoms were Dysphagia = 7, Throat pain = 6, FB sensation = 1 and Oral ulcer = 1. VLS was done for Diagnostic purposes in 7 cases and biopsy was done with VLS in all cases. VLS was done for follow-up in 8 cases. 3 patients were asymptomatic, and 5 patients were symptomatic with edema and residual growth.
Second primary
6 cases were diagnosed with second primary.
• Previous Carcinoma right Pyriform fossa T2 had growth on the left side of the epiglottis.
• Previous Carcinoma right buccal mucosa T3 had growth left pharyngoepiglottic fold
• Previous Carcinoma of the esophagus had a nodular lesion in the ventricular band
• 2 Previous carcinoma oral cavity after composite resection had growth in the posterior 1/3rd residual tongue.
• Previous Carcinoma posterior 1/3 rd tongue had growth in subglottis.
All cases underwent biopsy with videolaryngoscopy.
Discussion
In 1807, Philip Bozzini used an instrument called “lichtleiter” illuminated by a wax candle (2).
From that time on, different trials of laryngoscopy led to the revolution of videolaryngoscopy. Bastian et al. (3) concluded that Indirect Video Laryngoscopy can guide treatment planning (3). Pardal Refoyo and Munoz Navarro (4) validated videolaryngoscopy as indispensable in laryngeal changes (4). Al-Abbasi et al. (5) published three years of videolaryngoscopic experience in Iran (5). Yaseen (6) compared videolaryngoscopy with flexible fiberoptic laryngoscopy (6). Kaplan and Bryson (7) reviewed the evolution of laryngeal visualization by videolaryngoscopy (7). In September 2019 Shenson et al. (8) published Utility of videolaryngoscopy for diagnostic and therapeutic interventions in head and neck surgery (8).
In our study of 132 patients (Table 2), there were 92 (69.7%) male and 40 (30.3%) female patients 80% (104/132) of the population was in 40–60 years. Ogura and Spector (9) found a male-to-female ratio of 7:1 in the 6th decade and Kim et al. (10) found 6th–7th decade common.

Table 2. Master chart.
Overall symptoms of carcinoma larynx, hypopharynx, and oropharynx ranged from Dysphagia to Neck swelling. Dysphagia = 71, Voice change = 23, Throat pain = 19, Hoarseness = 14, Stridor = 7, Ear pain = 5, FB sensation = 2, Neck swelling = 1, Dyspnoea = 1, Oral ulcer = 1. Dysphagia is the most common symptom, even in laryngeal carcinoma (Figure 2).
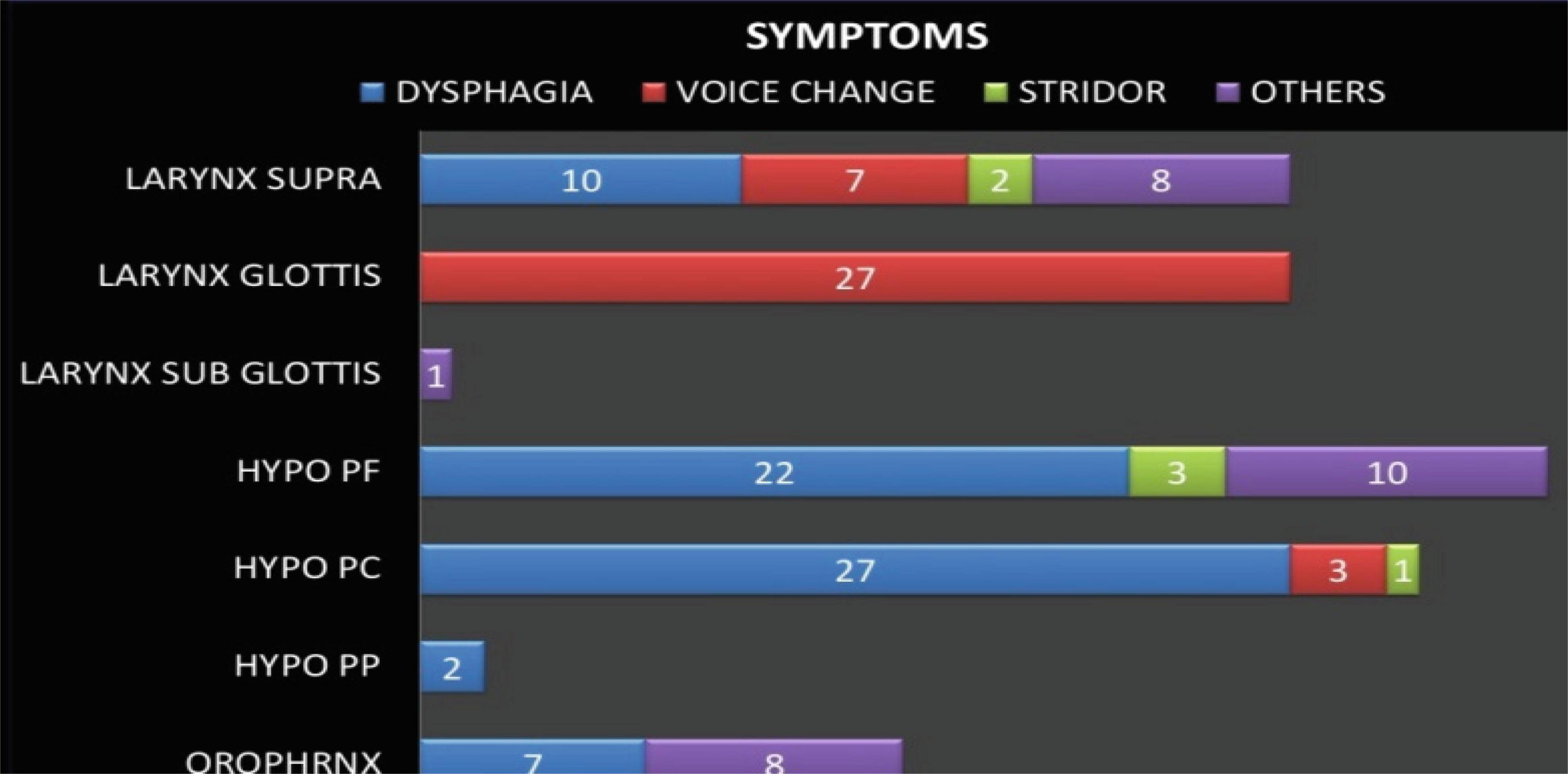
Figure 2. Symptoms of individual carcinomas (PF, pyriform fossa; PC, postcricoid; PP, posterior pharyngeal).
It is also reported similarly in other studies by Kukereja et al. (11) and Bhagat et al. (12). 61 patients had carcinoma hypopharynx, which was slightly more common than larynx.
The indication for videolaryngoscopy was Carcinoma hypopharynx in 61 (46.2%) patients, out of which 21 were for diagnostic, 40 for follow-up. Among hypopharyngeal lesions, 32 patients had lesions in pyriform fossa (52.5%), 27 patients had lesions in postcricoid (44.3%), and 2 patients had lesions in Post Pharyngeal wall (3.2%). In hypopharynx malignant lesions, lesions in Pyriform fossa are slightly commoner 13: 11 than post cricoid lesions. Saleh et al. (13), Zonunsangi et al. (14) found pyriform sinus as commonest while Verma et al. (15) found post cricoid commoner in hypopharyngeal malignancies.
54 patients who had carcinoma larynx (40.9%) underwent videolaryngoscopy, out of which 21 were for diagnostic and 33 for follow-up. Of all carcinoma larynx patients, 26 had supraglottis carcinoma (48%), 27 had glottis carcinoma (50%), and subglottis 1 (2%). Out of patients with supraglottis malignancy, 10 patients had lesions in ventricular band and 16 had lesion in epiglottis. Among laryngeal tumors, supraglottis cases were 26, almost equal to glottic, which was 27. Ogura and Spector (9) reported glottis (50–60%) and Fasunla et al. (16) reported transglottic as common. Glottis is reported as common in Western while in Indian studies, supraglottis is the most common (17).
15 patients who had carcinoma oropharynx involving the posterior 1/3rd tongue (12.9%) underwent videolaryngoscopy, out of which 7 were for diagnostic and 8 for follow-up.
6 patients (4.5%) had two primary lesions.
Among overall 132 laryngopharyngeal malignancy patients, 25 patients (17.8%) had T1 lesion, 48 patients (34.3%) T2 lesion, 47 patients (33.6%) T3 lesion, and 20 patients (14.3%) had T4 lesion (Figure 3).
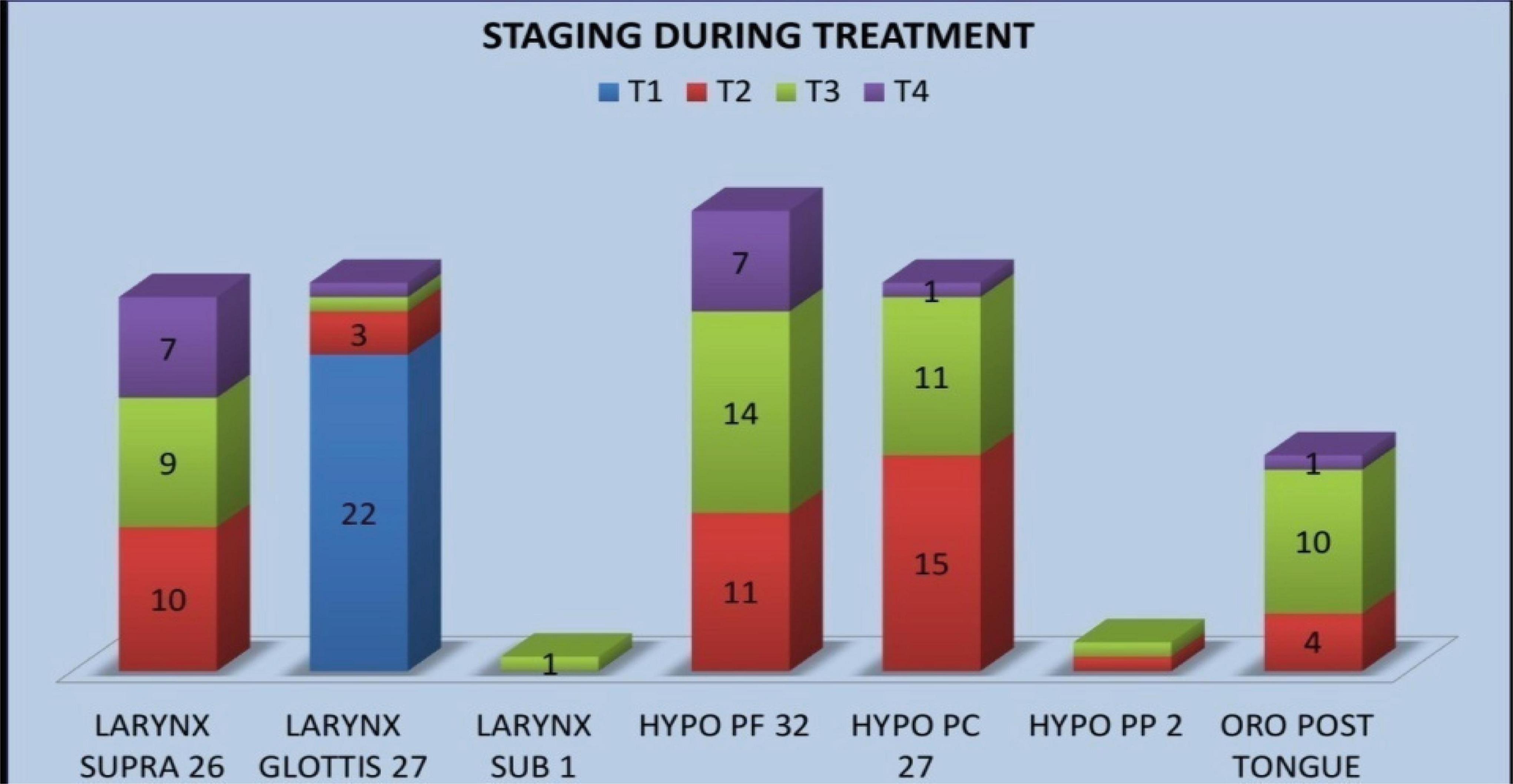
Figure 3. T staging at presentation (PF-pyriform fossa, PC-postcricoid, PP-posterior pharyngeal).
The overall purpose of videolaryngoscopy was Diagnostic in 56 cases out of which biopsy was done in 46 patients, 6 patients were advised microlaryngeal surgery, and 4 patients were advised UGI scope for biopsy of the lesion.
Among diagnostic VLS, glottic malignancy presented early 22 out of 27 (81%) had a T1 lesion. Of 32 pyriform fossa lesions 21 (66%) had T3 or T4 lesions. Among 15 posterior 1/3rd tongue malignancies, 11 (73%) patients presented late with T3 or T4 lesions. Second primary diagnosis was done in 6 patients.
The overall purpose of videolaryngoscopy was follow-up after radiotherapy and surgery in 81 cases. Of them 37 patients were asymptomatic with no recurrence or residual lesion. 44 cases were Symptomatic, of whom CT was advised for 13 patients, salvage surgery for 7 patients, biopsy of residual/recurrent lesion done for 3 cases. Tracheostomy had to be done in 2 patients and others were advised further follow-up as they were symptomatic.
Among all cases in follow-up after chemoradiotherapy, out of 22 cases of glottic malignancy 13 (58%) had no recurrent or residual lesions. Out of 8 oropharyngeal malignancies, 5 (63%) patients had symptomatic lesions (Figure 4).
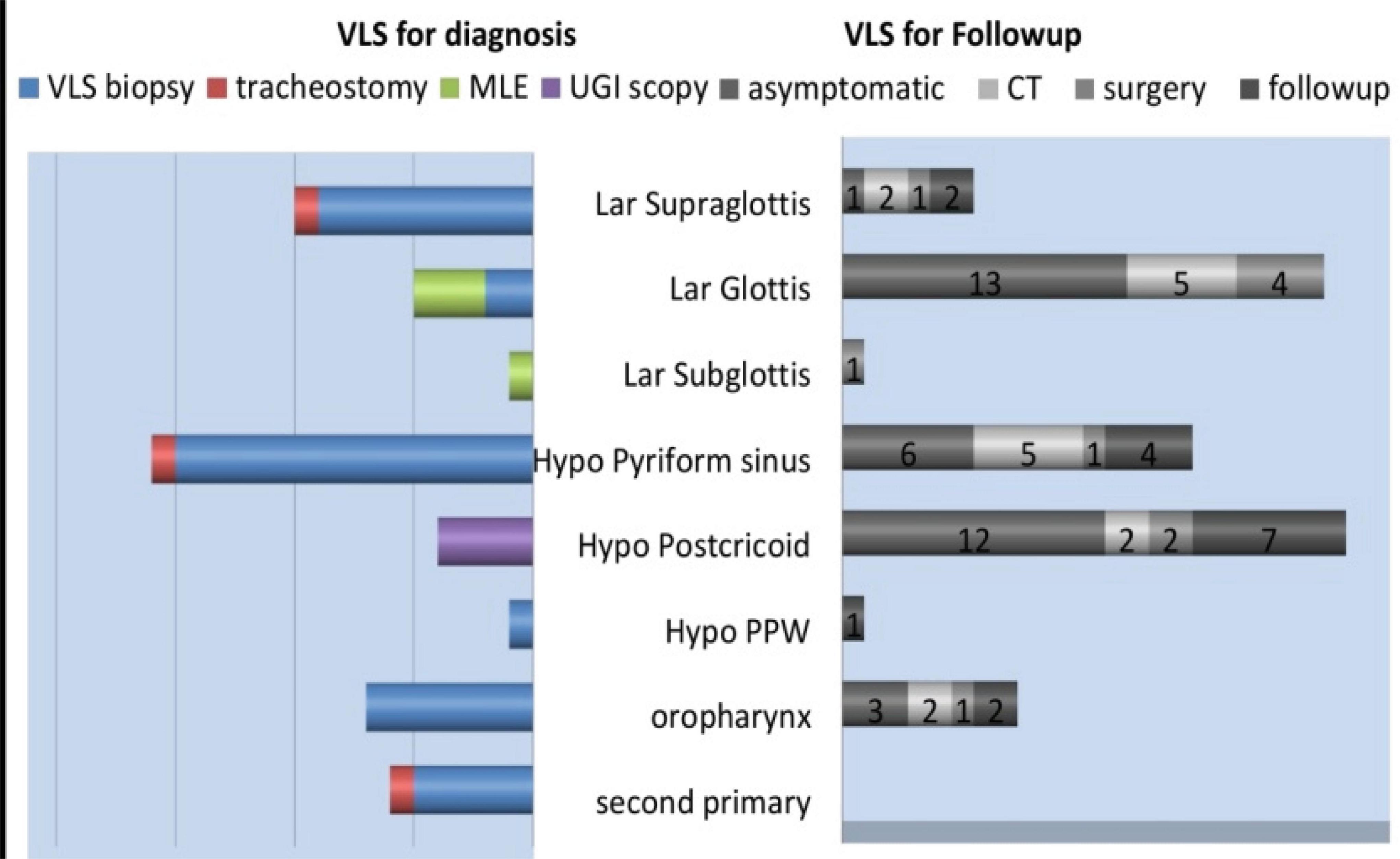
Figure 4. VLS outcome in carcinomas (VLS, videolaryngoscopy; MLE, microlaryngeal examination; UGI, upper gastrointestinal; CT, computed tomography; PPW, posterior pharyngeal wall).
Conclusion
As intended, the annual percentage prevalence of carcinoma larynx was 54 (40.9%), out of which supraglottis cases were 26 (48%), glottis 27 (50%), and subglottis 1 (2%). Carcinoma hypopharynx cases were 61 (46.2%), out of which pyriform fossa 32 (52.5%), postcricoid 27 (44.3%), and posterior pharyngeal wall 2 (3.2%). There were 15 oropharynx (11.3%) and 2 (1.6%) other malignancy patients. Videolaryngoscopy is a simple outpatient efficacious investigation in the diagnosis and follow-up of patients having carcinoma larynx, hypopharynx, and oropharynx.
References
1. International Agency for Research on Cancer.Global cancer observatory: Cancer today. Lyon, France. (2019). Available online at: https://gco.iarc.fr/today (accessed March 28, 2024).
2. Karmody C. The history of laryngology: ‘The larynx: A multidisciplinary approach. Boston, MA: Little, Brown (1988). p. 3–8.
3. Bastian R, Collins S, Kaniff T, Matz G. Indirect videolaryngoscopy versus direct endoscopy for larynx and pharynx cancer staging. Toward elimination of preliminary direct laryngoscopy. Ann Otol Rhinol Laryngol. (1989) 98:693–8. doi: 10.1177/000348948909800906
4. Pardal Refoyo J, Munoz Navarro C. Validity of videolaryngoscopy in detecting laryngeal structural changes. Ann Otorrinolaringol Ibero Am. (1996) 23:153–9.
5. Al-Abbasi AM, Sultan SSN, Witwit ML. Three years videolaryngoscopic experience in Basrah. Med J Babylon. (2006) 3:3–4.
6. Yaseen ET. Videolaryngoscopy by using 70 – degree 4 mm rigid sinuscope in comparison with flexible fiberoptic laryngoscopy. Iraqi J Commun Med. (2012) 4:357–62.
7. Kaplan SE, Bryson PC. Office procedures in laryngology office-based videoimaging of the larynx. Curr Otorhinolaryngol Rep. (2015) 3:132–7.
8. Shenson JA, Marcott S, Dewan K, Lee Y, Mariano ER, Sirjani DB. Utility of videolaryngoscopy for diagnostic and therapeutic interventions in head and neck surgery. Am J Otolaryngol. (2019) 41:102284. doi: 10.1016/j.amjoto.2019.102284
9. Ogura J, Spector G. “Management of the patient with cancer,” In: The larynx. Nelson TF editor. (Vol. 72), Philadelphia, PA: WB Saunders Company (1976). p. 206–38.
10. Kim M, Kim Y, Shim Y, Kim K, Chang H, Choi J, et al. Epidemiologic survey of head and neck cancers in Korea. J Korean Med Sci. (2003) 18:80–7. doi: 10.3346/jkms.2003.18.1.80
11. Kukereja A, Varshney S, Gupta N, Harsh M, Bist S, Bhagat S. Clinical profile of pharyngeal malignancy in a tertiary care centre, state of Uttrakhand. Indian J Otolaryngol Head Neck Surg. (2013) 65:53–65. doi: 10.1007/s12070-012-0481-1
12. Bhagat S, Singh B, Verma S, Singh D, Bal M. Clinic-pathological study of tumors of hypopharynx. Indian J Otolaryngol Head Neck Surg. (2003) 55:241–3. doi: 10.1007/BF02992428
13. Saleh E, Abdullwahab A, Kammal M. Age and sex incidence of hypopharyngeal tumors in upper Egypt: Assult university experience. J Laryngol Otol. (1995) 109:737–40. doi: 10.1017/s0022215100131184
14. Zonunsangi, Sobita P, Sudhiranjan T, Malik P, Tenzing JB, Konyak SY. Etiopathological factor, clinical presentation and management of hypopharyngeal malignancies. Indian Med Gazette. (2014) 27:271–5.
15. Verma A, Mehta S, Panda N, Mann B, Mehra Y. Presentation of carcinoma larynx and hypopharynx- an analysis of 840 cases. Indian J Otolaryngol. (1990) 42:50. doi: 10.1007/BF02993189
16. Fasunla A, Ogundoyin O, Onakoya P, Nwaorgu O. Malignant tumors of the larynx: Clinicopathological profile and implication for late disease presentation. Nigerian Med J. (2016) 57:280–5. doi: 10.4103/0300-1652.190596